Good morning, Thread Readers.
“Nearly one in three U.S. women over 40 experiences severe menopause symptoms, and those symptoms can be severe enough to disrupt daily life. For many women, menopause means waves of depression they’ve never experienced before or terrible insomnia. The underlying hormonal changes driving these symptoms increase a woman’s risk of cardiovascular disease, osteoporosis, and certain types of cancer.”
— Melinda French Gates in the New York Times
Two bipartisan bills in the 119th Congress aim to improve the care and disparity in funded research that over half the population so richly deserves. Sen. Patty Murray (D-WA) and Sen. Joni Ernst (R-IA) lead the Servicewomen and Veterans Menopause Research Act (S. 1320 / H.R. 2717), joined in the House by Reps. Chrissy Houlahan (D-PA) and Stephanie Bice (R-OK). Sen. Murray and Sen. Lisa Murkowski (R-AK) lead the Advancing Menopause Care and Mid-Life Women's Health Act. The first builds the evidence base for women who served. The second funds research, trains providers, and coordinates the federal response for every woman in midlife.
Let's dig in.
The gap starts with one study: the 2002 Women’s Health Initiative. Its findings triggered a near-total collapse in hormone therapy prescribing. Use fell from roughly 40% of postmenopausal women to under 4%. Providers were told, and told patients, that hormone therapy was dangerous.
Here is what the study got wrong: the women enrolled had an average age of 63, nearly a decade past the typical onset of menopause, and many were already at elevated cardiovascular risk. The FDA now points to randomized data showing that women who start hormone therapy within 10 years of the onset of menopause, generally before age 60, see lower all-cause mortality and fewer fractures.
In late 2025, the FDA moved to reverse more than two decades of guidance, and in February 2026 it approved the first label changes, stripping the boxed warning, its most serious safety label, from the initial batch of hormone therapy products. Former FDA Commissioner Marty Makary called the long stretch of fear around hormone therapy “an American tragedy” and estimated that 50 to 70 million women had been denied “life-changing, life-saving benefits” because of it.
The science has changed. Federal policy has not caught up.
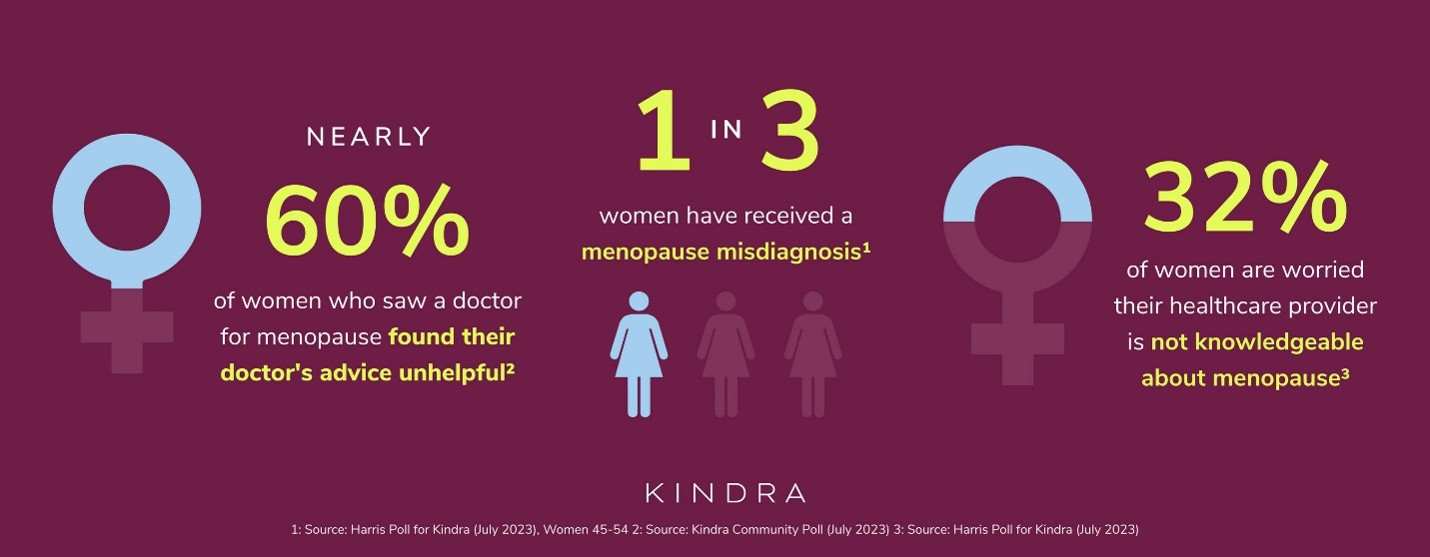
Key data:
Solutions
The two bills are built to work together. Between them, they take on what two decades of neglect left behind: too little research, too few trained providers, and no coordinated federal response.
The research foundation: The Servicewomen and Veterans Menopause Research Act
S. 1320 / H.R. 2717 — Murray (D-WA), Ernst (R-IA) | Houlahan (D-PA), Bice (R-OK)
The Servicewomen and Veterans Menopause Research Act directs the Departments of Defense and Veterans Affairs to evaluate existing research on menopause among active-duty servicewomen and women veterans, map what remains unknown, and deliver a strategic plan to fill it.
Women who serve face risks the general population does not. PTSD and chronic stress are linked to earlier menopause and more severe symptoms. The “forever chemicals” known as PFAS, used for decades in the firefighting foam on military bases, interfere with the body's hormones and have been tied to earlier menopause in peer-reviewed research. Published VA data also documents racial disparities in who gets care within the system.
In December 2025, the Senate Veterans’ Affairs Committee took a real step forward after the bill stalled at the close of the 118th Congress, reporting it out of committee. Joining Sens. Murray and Ernst as Senate cosponsors are Sens. Bill Cassidy (R-LA), Kirsten Gillibrand (D-NY), John Hickenlooper (D-CO), Jim Justice (R-WV), Angus King (I-ME), Amy Klobuchar (D-MN), Jerry Moran (R-KS), Jon Ossoff (D-GA), and Jeanne Shaheen (D-NH). In the House, Reps. Houlahan and Bice were joined by Reps. Wesley Bell (D-MO), Donald Davis (D-NC), Cleo Fields (D-LA), Brian Fitzpatrick (R-PA), Maggie Goodlander (D-NH), Michael Guest (R-MS), David Joyce (R-OH), Ted Lieu (D-CA), Seth Moulton (D-MA), Andrea Salinas (D-OR), and Jill Tokuda (D-HI). In addition, a companion House bill, the Improving Menopause Care for Veterans Act (H.R. 219), led by Representative Julia Brownley (D-CA) with 35 House cosponsors, directs the GAO to independently assess which menopause services the VA is delivering and then requires a plan to improve access.
The care expansion: The Advancing Menopause Care and Mid-Life Women’s Health Act
S. 4503 — Murray (D-WA), Murkowski (R-AK)
Seventeen (17) women senators backed this bill in the 118th Congress. Bipartisan co-leads brought it back this year. Authorized at $275 million over five years, it would:
Growing Support
Both bills have backing from veterans service organizations, including Iraq and Afghanistan Veterans of America, Disabled American Veterans, and the Military Officers Association of America, alongside The Menopause Society, the Society for Women's Health Research, and the American College of Obstetricians and Gynecologists.
Bills like these rarely pass in a single Congress. In the 118th Congress, Rep. Diana Harshbarger (R-TN) and then-Rep. Lisa Blunt Rochester (D-DE) (now Senator) introduced the We're Addressing the Realities of Menopause Act, known as the WARM Act, a bipartisan House bill to fund a national menopause awareness campaign and help providers recognize and treat it. The WARM Act did not become law, but it put menopause on the federal agenda and laid the groundwork for the bills moving now. Blunt Rochester has since moved to the Senate, where this fight continues. Regular Thread readers know how this goes: a bill becomes law because a handful of members refuse to drop it, reintroducing it in Congress after Congress until it finally moves, for the women back home who are counting on it.
The states are moving too. By mid-2025, 19 had introduced more than three dozen menopause bills. Rhode Island became the first state to pass a law requiring workplace accommodations for menopause-related conditions. Four states now require insurance to cover menopause treatment.
Facts Be Told
We say it every issue, and we will keep saying it: this is a women's economic security issue. When a woman cannot get care, she pays for it in her paycheck, in her savings, and in the years she can stay in the workforce. A 2025 Stanford study found that women who seek help for menopause symptoms earn 10% less four years later, and untreated symptoms drain an estimated $26.6 billion from the economy each year, $1.8 billion of it in lost productivity alone. The care is often not there, even when women go looking for it. The Menopause Society counts about 1,300 certified menopause specialists for roughly 50 million American women in perimenopause or menopause, one specialist for every 38,000 women. Closing that gap is the mission of these bills.
The following leaders are bringing real bipartisan commitment to menopause and midlife women's health and are leading these bills forward, proof that the best teams play across every line, on the Hill and on the pitch:
Curaçao, Cape Verde, and Congo DR. ⚽❤️
And there is also this:
“The Mayo Clinic estimates that menopause-related symptoms cost the United States $26 billion in medical expenses and lost work time every year.”
— Melinda French Gates in the New York Times
Engage is excited to gather over 20 bipartisan, bicameral staff for the third convening of our Menopause & Longevity working group for lunch on Monday. On the agenda is this legislation and more! If you want to learn about Engage's work in this area, we would love to hear from you.
Be kind to one another.
The next issue of The Thread will be out on July 11th.